-Pradeep Neupane

Laboratory
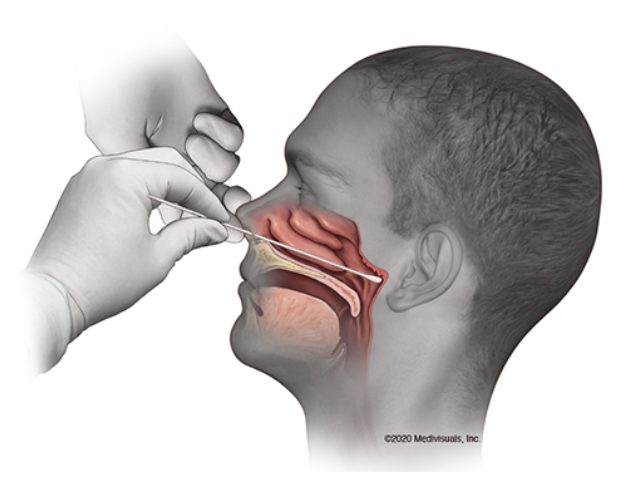
diagnosis of human coronavirus (COVID-19 virus/SARS-CoV-2) infection mainly
relies on detection of viral RNA in clinical samples by “gold standard” reverse
transcription polymerase chain reaction (RT-PCR) or detection
of viral proteins or viral-specific antibodies (IgM/IgA/IgG) by serological
immunoassays (rapid diagnostic tests (RDT)). None of these tests has
100% diagnostic accuracy.
Although
RT-PCR is a highly sensitive and specific, it generates numerous false negative
results meaning persons with active COVID-19 infection may test negative. Recent
studies indicate that relying solely on RT-PCR to diagnose the virus infection is
a risky strategy. CoVID-19 viral loads may vary considerably in various types
of respiratory samples from the same patient. Given the variability of viral RNA
loads in clinical specimens, RT-PCR detection may miss some true cases due to low
viral loads or sampling variability. The accuracy of test results is dependent
on the integrity of specimens. RT-PCR is dependent on procuring high-quality
RNA from respiratory samples. Improper collection and handling of clinical specimens
can affect the quality of the sample and hence the outcome of the test results,
particularly RT-PCR results. Erroneous results as a result of specimen mismanagement
compromise the care of patients and hamper the efforts to curb the global CoVID-19
pandemic.
On
the other hand, antibody-detecting RDT show some advantages over RT-PCR.
IgM/IgA/IgG serological tests are used to detect anti-viral antibodies in serum
(blood) that are produced by host immune system in response to the viral
infection. Antibodies are more uniformly distributed in blood. IgM/IgA/IgG are considerably
more stable than RNA, which makes IgM/IgA/IgG less susceptible to degradation during
sample collection, handling, storage, and transportation. One of the major advantages
of serological assay is that it can detect past infection since IgM/IgA/IgG (primarily
IgG) can persist in the bloodstream for several weeks/months/years after the infection.
It is unclear whether recovered CoVID-19 patients are immune to reinfection
from CoVID-19. In other word, there is no evidence that antibodies provide
protection against the CoVID-19 virus. Many components of host innate immune system
including T helper cells, NK and/or cytotoxic CD8 T cells may play important roles
in protecting against CoVID-19.
Serological tests have several limitations
including the following: 1) Antibodies are produced over days to weeks after initial
infection, suggesting positive serological test result might not be indicative of
active CoVID-19 infection; 2) Virus specific IgM/IgG antibodies may not be
detected at least 7 to 11 days after infection since IgM and IgG antibodies response
against CoVID-19 virus does not peak until ~9 and ~11 days after infection, respectively; 3) Presence of cross-reacting
antibodies in serum (blood) from previous infections with other non-CoVID-19
human coronaviruses may result in false-positive test.
In conclusion, RT-PCR and serological assays, commonly
used tests to diagnose the CoVID-19 infection, are often unreliable, generating
erroneous test results. Although RT-PCR is the most frequently used “gold-standard”
method for diagnosis of CoVID-19 infection, results of RT-PCR must be cautiously
interpreted. Therefore, antibody detecting RDT should also be taken into
consideration and their results in conjunction with RT-PCR can be invaluable in
providing rapid diagnosis of CoVID-19 infection. Also, antibody testing will be
crucial for accurate determination of serological immunity levels amongst
populations and for investigating optimal strategies to control the spread of CoVID-19.
References
Liu, L.,
Liu, W., Wang, S. and Zheng, S., 2020. A preliminary study on serological assay
for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in 238
admitted hospital patients. medRxiv.
Li, Z., Yi,
Y., Luo, X., Xiong, N., Liu, Y., Li, S., Sun, R., Wang, Y., Hu, B., Chen, W.
and Zhang, Y., 2020. Development and clinical application of a rapid IgM‐IgG
combined antibody test for SARS‐CoV‐2 infection diagnosis. Journal of medical virology.


























.jpg)